Patellofemoral pain syndrome (PFPS) is one of the most common 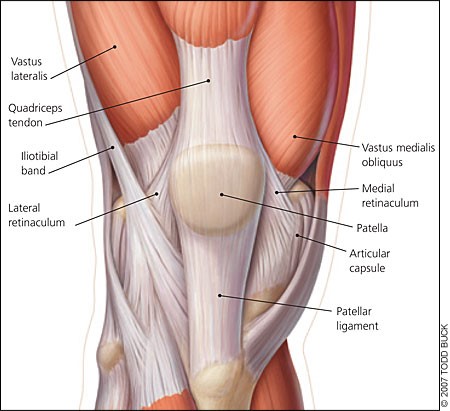 musculoskeletal injuries suffered in the adult population. PFPS accounts for approximately 25% of all identified knee injuries and nearly 10% of all visits to musculoskeletal and orthopaedic clinics. This condition is sometimes referred to as “runner’s knee” but is also seen in the sedentary population.
musculoskeletal injuries suffered in the adult population. PFPS accounts for approximately 25% of all identified knee injuries and nearly 10% of all visits to musculoskeletal and orthopaedic clinics. This condition is sometimes referred to as “runner’s knee” but is also seen in the sedentary population.
This diagnosis covers a range of symptoms in, under or behind the knee cap due to poor biomechanical loading to the structures in this area. Structures involved can include the retro patella cartilage, infrapatella fat pad and occasionally the patella tendon. Typically, patients complain of pain with running and walking, descending stairs, deep squat and after periods of prolonged knee flexion such as with sitting.
PFPS patients typically present with poor strength or recruitment of hip external rotators, tight lateral structures of the hip and thigh, delayed onset of vastus medialis oblique (VMO) firing seen on EMG study and proprioceptive dysfunction.
 Correct patellofemoral tracking is reliant on the balance of the medial and lateral static and dynamic patellofemoral stabilisers. It is suggested that the VMO helps to hold the patella in position by applying a medial force to counteract the lateral pull of the vastus lateralis (VL) muscle. The trend in the literature suggests that in PFPS patients, the patella tracks and tilts laterally, however data to support this is inconsistent.
Correct patellofemoral tracking is reliant on the balance of the medial and lateral static and dynamic patellofemoral stabilisers. It is suggested that the VMO helps to hold the patella in position by applying a medial force to counteract the lateral pull of the vastus lateralis (VL) muscle. The trend in the literature suggests that in PFPS patients, the patella tracks and tilts laterally, however data to support this is inconsistent.
Recent evidence points to weakness of the hip as the underlying driver of the dysfunction. The truth of the matter is likely that there is no one mechanism resulting in PFPS, but more so several maladaptive biomechanical patterns that may overload tissue in this area. These patterns may develop for a number reasons from weakness of stabilizing muscles of the lower limb to simply adopting poor gait patterns consciously or subconsciously.
Evidence has shown that in the presence of patellofemoral pain, VMO activation is delayed in relation to VL activity in a range of functional weight bearing activity. Physiotherapy comprising VMO retraining with EMG biofeedback, gluteal strengthening, release of tight iliotibial band and lateral structures of the hip in conjunction with patella taping, has been shown to very effective in treatment of the condition. This should be carried out with appropriate activity modification and biomechanical correction for lasting results.
In Balance Physio and Pilates utilizes the latest research and technology in diagnosis and treatment of patellofemoral pain syndrome. Patients are assessed using video motion analysis software, EMG traces and utilise EMG biofeedback for VMO retraining. In keeping with the philosophy of the practice this is always undertaken with correction of underlying biomechanical and postural issues.
Article by Jim Burke
