Anterior cruciate ligament (ACL) tears are a common injury, particularly in the athletic population. For many years the doctrine taught, and message passed onto patients was that while conservative management of these injuries was possible, without surgery, their knee would always be unstable and prone to early onset osteoarthritis and meniscal tears. The thinking at the time was that at best, successful conservative management would require significant lifestyle restrictions and that if they wished to return to sport, that ACL reconstruction surgery was really their only option.
Underpinning this advice was the belief that once ruptured, the ACL could not possibly heal. In recent years, there has been growing evidence for the possibility of successful conservative rehab of full and partial ACL tears, with a significant number returning to high level sports like skiing and rugby, without a significant difference in success rate between surgical repair and conservative management. Most of the success of this approach had been put down to a very thorough rehab program, building good strength and control of the muscles around the knee.
More recently, there has been research following full and partial thickness tears managed conservatively to see if there is the possibility of the tendon healing. While the studies to date have only been quite small, there has been some exciting results. The recent KANON study followed 120 young active participants with acute ACL tears. They were assigned into early surgery and rehab or rehab with the option of delayed surgery. The study found there was no significant improvement in outcomes for those who delayed surgery compared to those who underwent early surgery but more interestingly, the study found that of the participants who chose not to have the surgery at all, 58% showed proof of ACL healing at 5 year follow up. (10)
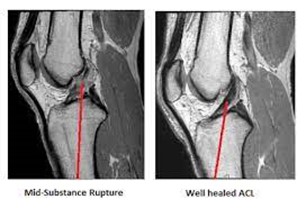
These results appear to be backed up by several other studies which have shown the possibility of full thickness ACL tears healing under several different approaches including bracing, rehabilitation and strengthening and even with no intervention at all (8,9). Another recent study has suggested that the rate of subsequent meniscal tears in the knee may even be greater in reconstructed knees than in those managed conservatively! (26,27)
So, should we stop advising people to have their ACL repaired? The decision to manage surgically or conservatively is a very personal one. At the very least we need to educate people that the most recent research seems to have thrown doubt on many long-held beliefs. There seems to be good evidence that at worst, there does not appear to be any significant difference in outcomes and return to function for conservative management over surgery and trialling conservative rehab is certainly a viable option. At best, there may be growing evidence for superior outcomes with conservative management. No doubt further research needs to be done but watch this space.
