Article by Jim Burke
Vertigo is the sensation that objects around you are moving when they are not. The most common type of vertigo is known as Benign Paroxysmal, Positional Vertigo or BPPV for short. Sensory information about motion, equilibrium and spatial orientation is provided by the vestibular apparatus, which in each ears includes the utricle, saccule and 3 semicircular canals. These semicircular canals are oriented at right angles to one another and contain a liquid called endolymph. When the head rotates in the plane of one of these canals, the endolymph in the canal lags behind due to inertia and exerts pressure on the canals sensory receptors, which in turn fire off a message to the brain that the head is moving in a particular direction.
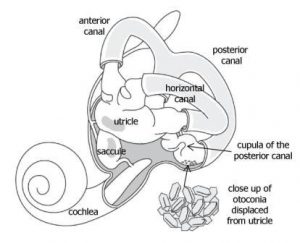
BPPV occurs when some of the calcium carbonate crystals (otoconia) that are normally embedded in gel in the utricle, become dislodged and migrate into one or more of the 3 fluid filled semicircular canals. When enough of these particles accumulate in one of the canals, they interfere with the normal fluid movement that these canals use to sense head motion, causing the ear to send false signals to the brain. When the information from the eyes and from the vestibular system do not match up, the result is the sensation of vertigo. BPPV symptoms vary between individuals and depend on which of the canals are effected but typically, symptoms are elicited by rolling in bed, turning the head and looking up and the dizziness may be accompanied by a sensation of nausea. The symptoms are generally fairly short lived, generally settling within a minute.
BPPV is fairly common, effecting about 1 in 1000 people per year, with a lifetime prevalence of about 2.5% (2). The vast majority of cases occur for no apparent reason, with many people reporting onset of symptoms after getting out of bed and feeling the room begin to spin. There have been associations made between BPPV and trauma, migraine, inner ear infection. There may also be correlation with the side people sleep on. These correlations are not well understood.
Diagnosis of BPPV is made with specific tests that are designed to move the dislodge crystals within the canal. A positive test will cause the eyes to move in a very specific pattern called nystagmus. Treatment of BPPV in the vast majority of cases involves using gravity to reposition the crystals in the correct position in the utricle via a series of simple but very specific, mechanical movements of the head and neck called canalith repositioning manoeuvres. The most widely known procedure is the Epley manoeuvre. Generally, treatment success is quite good, with 90% of patient’s symptoms resolving within 1-3 treatments. Unfortunately, 50% of these people will suffer some sort of re-occurrence within a 5 year period.
